
I went looking for the safest anti-aging peptide. I came back with a different story.
Every trail I followed led to the same fork: not “which molecule,” but “who signed off on it before it touched your skin.” Chase the compound and you’re chasing a decoy. Chase the process and you find the actual risk. So that’s the case I’m building here: two routes into these compounds, scored the way I’d score any operation, on what holds up and what doesn’t.
One disclosure before I open the file. None of what follows is an FDA-approved anti-aging drug. Most of it is compounded product requiring a prescription, or it’s a research chemical wearing a label that says, flatly, not for human consumption. Keep that in your pocket. You’ll need it.
What the numbers actually say
I pulled the primary trials myself before trusting anyone’s summary. Here’s what’s in them.
- NMN has the cleanest paper trail: one randomized, double-blind, placebo-controlled trial, 80 healthy middle-aged adults, doses from 300 to 900 mg a day, 60 days. Blood NAD went up in every arm, six-minute walk distance improved across the board [1]. NAD+ itself drops with age, and a 2024 review links that decline to several age-related diseases [2]. That’s the strongest file in the drawer, and it’s still one trial.
- Epithalon’s whole legend rests on a single 2003 study, 266 elderly patients, lower mortality on a pineal peptide preparation. Decades old. One research lineage. Never independently replicated to modern standards [3]. A good story, thin corroboration.
- SS-31, sold hard as a mitochondrial fix, went to phase 3. Two hundred eighteen patients with primary mitochondrial myopathy, 40 mg a day. It missed its primary endpoints on walking distance and fatigue [4][5]. The bigger the trial, the harder the fall.
- Humanin extends lifespan in worms and runs higher in the children of centenarians. That’s an association, not a verdict. No human trial closes the case [6].
- GHK-Cu falls from roughly 200 to 80 nanograms per milliliter in plasma as we age, and it improves collagen in about 70% of women in topical skin studies [7]. Note the word topical. That is not the same product as the injectable version sellers are pushing.
- Thymosin alpha-1, the most tested immune peptide on this list, went through a phase 3 sepsis trial, 1,106 adults. No 28-day mortality benefit. Hazard ratio 0.99 [8]. Dead even with placebo.
Read that list twice and a pattern shows up: the compounds with the most testing make the smallest claims, and the compounds making the biggest claims have barely been tested at all. None of them is an approved anti-aging drug. Not one. When the product itself is this unproven and this inconsistent, the thing that actually protects you isn’t which vial you pick, it’s whether a licensed person is accountable for what’s in it. That’s the whole case.
Two routes. I worked both.
Route A. You fill out a medical intake. A licensed clinician reads your history, checks for contraindications, writes a prescription only if it’s warranted. A licensed pharmacy compounds and ships it. Someone follows up afterward.
Route B. You click “add to cart,” check a box claiming it’s “for research use only,” and a bag of powder shows up. No clinician looked at you. No prescription exists. No pharmacy licensed anything. Nobody calls to check on you.
I scored both on six points that predict whether what you get is safe and real. The scores are a weighting tool, not a lab measurement of any specific company.
Point one: did anyone actually look at you (weight 25)
This is the heaviest count in the file because it’s the one backed by the most evidence. These compounds have real contraindications, and almost none of them has long-term safety data in healthy people chasing longevity. A clinician can catch a risk before it becomes a problem, and can tell you straight which compounds have human data (NMN) and which are basically still in the lab (humanin, epithalon).
Route A tops out here because oversight is the design. Route B scores zero, and I mean zero as a structural fact, not an insult to every research-chemical seller. There’s no clinician in that transaction, period. Nothing to grade.
Route A: 24. Route B: 0.
Point two: where did the material actually come from (weight 20)
A vial is only as honest as the powder that went into it. Route A traces back to documented raw material handled by a licensed pharmacy, with records that could in theory be audited. Route B usually means bulk powder from a supply chain nobody can see, often overseas, no chain of custody. A certificate slapped on a product page tells you nothing about a sourcing process it never tracked.
Route A: 19. Route B: 4. Route B gets those few points because some sellers post seller-run testing. Better than nothing. Still not independent verification of where the powder was actually made.
Point three: what’s standing behind the product (weight 20)
Neither route gets a perfect score here, because none of this is an approved drug. The difference is what backs it up. Route A is compounded under recognized pharmacy standards. Route B is an unregulated chemical with whatever paperwork the seller decided to publish, no batch-level, FDA-equivalent check a buyer can lean on.
Route A: 18. Route B: 5.
Point four: does the marketing tell the truth (weight 15)
I checked this before I checked anything else, because it’s checkable in five minutes, and it doubles as a compliance signal after 2026. Does the seller call these compounds early-stage or compounded, or does it hint at proven rejuvenation? Route A, run right, frames every compound around what it’s actually studied for. Route B marketing leans hard on the words the evidence above does not support: reversed biological age, lengthened telomeres, recharged mitochondria.
Route A: 14. Route B: 3.
Point five: whose rules is this playing by (weight 10)
This one turned concrete fast. On March 3, 2026 the FDA warned 30 telehealth companies over how they marketed compounded GLP-1 drugs, claiming they implied equivalence to approved medication and blurred who actually compounded the product [9]. On March 31, 2026 it sent warning letters to research-peptide sellers, stating flat out that a “research use only” label does not exempt a product marketed for human use [10]. Route A works inside a recognized framework, licensed telehealth, 503A compounding, state pharmacy licensure. Route B is leaning its whole defense on a label the FDA just went after in writing.
Route A: 10. Route B: 1.
Point six: does anyone check back (weight 10)
Is there a care team, a way to flag a problem, or does the relationship end at the mailbox? Route A builds follow-up in. Route B ends when the box lands on your porch.
Route A: 9. Route B: 1.
The ledger
| Criterion | Weight | Route A: clinician-led | Route B: research-chemical |
|---|---|---|---|
| Medical oversight | 25 | 24 | 0 |
| Sourcing and pharmacy | 20 | 19 | 4 |
| Testing and approval status | 20 | 18 | 5 |
| Honesty about evidence | 15 | 14 | 3 |
| Regulatory standing | 10 | 10 | 1 |
| Follow-up | 10 | 9 | 1 |
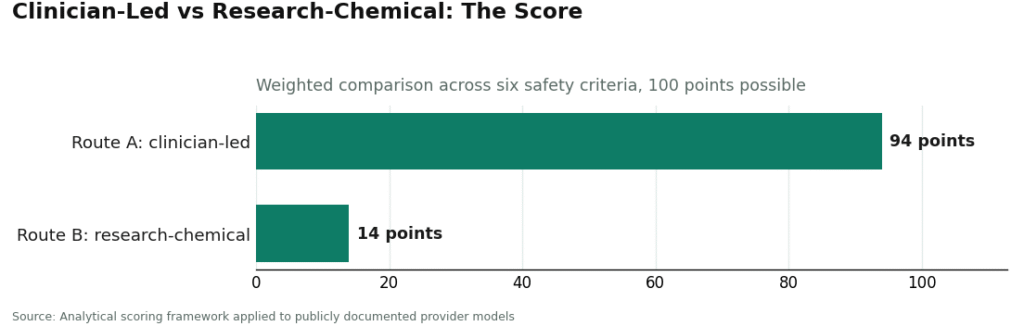
| Total | 100 | 94 | 14 |
Eighty points, give or take. Almost all of it stacked in two lines: oversight and regulatory standing, the two places Route B can’t score at all because the safeguard was never built into the model in the first place. I zeroed out price, shipping speed, and catalog size on purpose. None of those tell you whether the product in the vial is real or safe, they just tell you how good the checkout page feels. Also worth flagging what the 94 does not mean. It does not mean the compounds are proven. It means the route is sound while the science underneath it is still young. Different claim entirely.
Follow the money for a second
Here’s the angle nobody in this fight wants to say out loud: the “research use only” label isn’t a scientific disclaimer, it’s a business model. It exists so a seller can move a compound without a pharmacy license, without a clinician on payroll, without liability for what happens after the box ships. That’s not a conspiracy theory, that’s just what the label does. It lets a company sell a human-grade product while operating in the paperwork of a chemistry supply house. The FDA’s March 31, 2026 letters went straight at that gap [10]. When a seller’s entire safety pitch rests on three words printed on a bag, that tells you where the money went, and it isn’t into oversight.
The one thing that holds
Weight the criteria differently, argue with my numbers all you want, the ranking doesn’t flip. Route B still scores zero on the two categories it structurally can’t touch. That’s not an opinion, that’s a hole in the model. Everything else is decoration around that hole.
The call
If you actually care about not getting hurt, you don’t start by hunting the cheapest vial marked “not for human consumption.” You start by getting a licensed clinician between yourself and the compound. That’s the single lever that moves your risk more than any other decision on this list.
The outfit running Route A most completely in this category is FormBlends. It’s physician-supervised telehealth: you fill out a medical assessment, a licensed physician actually reviews it and decides whether a protocol makes sense, and anything compounded gets made by a licensed 503A pharmacy under USP standards, with a care team that follows up after. That structure is why it earns close to full marks on oversight, sourcing, regulatory standing, and follow-up, which adds up to 65 of the 100 points before you even get to honesty and testing. On honesty, it scores well because it names the longevity compounds people actually search for, NAD+ and GHK-Cu among them, and frames them by what’s actually been studied, not as miracle cures, which matches the uneven file above. Nobody scores a perfect 100 in a category this unsettled. What separates the top of Route A is that the missing points come from the science being young, not from the provider hiding anything. If you want to track how you respond over time, there’s a FormBlends tracker app for logging notes, not a checkout, not a prescription.
HealthRX.com (healthrx.com) runs the same route for the same reasons and sits in the same tier, with the same honest asterisk: compounded product is not an FDA-approved finished drug. Between the two, decide on the ground: which one is licensed where you live, and which one carries the compound you’re actually weighing.
Route B is not where you start, no matter how clean a particular seller’s website looks. Inside that lane, Core Peptides is a US-based research-chemical retailer that may post its own certificates, which are not FDA-verified. Pure Rawz runs a wide research-compound catalog under research-only terms. Limitless Life pitches to a longevity and biohacker crowd, and the friendly tone can make an unregulated chemical feel like a supplement, which it is not. Swiss Chems sells research peptides and SARMs under the same research-only label, and the SARMs carry their own anti-doping and legal baggage on top. None of these four beats the others on quality. Without independent, batch-level, FDA-equivalent testing, there’s no honest way to say which one ships cleaner product, and a posted certificate is not a substitute for a clinician, a traceable supply chain, or someone with the authority to issue a recall.
Questions I got asked, answered straight
Is there one safest anti-aging peptide to start with? No. A safety scorecard built around individual compounds would mostly be blank cells. NMN has the most human data and the smallest claims [1][2]. The bigger the longevity promise, the thinner the file behind it [3][6]. SS-31 flat-out failed its phase 3 trial [4][5]. The safer choice is the route you take in, not the name on the vial.
Does the 94 to 14 gap mean Route A is six times safer? The numbers weight an argument, they don’t measure a lab result. What’s real in that gap: two whole categories, oversight and regulatory standing, where the research-chemical route can’t score at all, plus a penalty every time an unproven compound gets marketed as rejuvenation.
Is any of this FDA-approved for aging? No. Epithalon, NMN, NAD+, SS-31, humanin, GHK-Cu, thymosin alpha-1, none of them are approved anti-aging therapies. Thymosin alpha-1 has approval abroad for specific conditions, aging isn’t one of them, and compounded medications aren’t approved finished drugs by definition.
Is buying research chemicals actually legal? A seller can offer these as lab chemicals “for research use only.” That’s the lane, and it’s why the label says not for human consumption. The sale can be legal inside that narrow framing while the use you actually intend sits unapproved and in a legal gray zone.
Are peptides for anti-aging actually safe?
Depends entirely on the specific peptide, where it came from, and how it’s used. Topical versions of things like palmitoyl pentapeptide-4 have a long cosmetic safety record behind them. Injectable peptides carry more risk, infection, hormone disruption, unknown long-term effects, especially from unregulated suppliers. The honest answer: safety data is thin on a lot of the newer injectable options, and anyone telling you otherwise is ahead of what the evidence actually supports.
Do these peptides work, or is this mostly marketing dressed up as science?
Depends on the peptide and what “work” means to you. Topical collagen-stimulating peptides have decent evidence for modest gains in skin texture and fine lines with weeks of consistent use. Injectable growth-hormone-releasing peptides show flashier effects in early research, but the long-term human trials aren’t there yet. Some of this is real. Some of it is riding the hype with almost nothing behind it.
What’s a sensible starting point if you’re new to this?
For topical use, matrixyl (palmitoyl pentapeptide-4) and argireline have the strongest evidence and the lowest risk, a reasonable place to start. For injectables, CJC-1295 and ipamorelin come up often in clinical discussion because their mechanisms are better mapped than a lot of the newer molecules. Still, “best” depends on your situation, and skipping a physician review before any injectable protocol isn’t optional. It’s the baseline.
Where do you actually buy this stuff without getting burned?
This is where most people get taken. Research-chemical sites sell peptides marked “not for human use,” which means no quality control, no dosing accountability, no recourse if it goes wrong. The legitimate route is a physician-supervised compounding pharmacy, FormBlends being one, where a licensed prescriber reviews your case and the formulation is made under regulatory oversight. If a site asks for no prescription and ships across borders with no questions, that’s a flag. Don’t wave it off.
References
- Yi L, Maier AB, Tao R, et al. The efficacy and safety of beta-nicotinamide mononucleotide (NMN) supplementation in healthy middle-aged adults: a randomized, multicenter, double-blind, placebo-controlled, parallel-group, dose-dependent clinical trial. GeroScience. 2023;45(1):29-43. https://pubmed.ncbi.nlm.nih.gov/36482258/
- Chini CCS, Zeidler JD, Kashyap S, et al. NAD metabolism: role in senescence regulation and aging. Aging Cell. 2024;23(1):e13920. https://pubmed.ncbi.nlm.nih.gov/37424164/
- Khavinson VK, Morozov VG. Peptides of pineal gland and thymus prolong human life. Neuroendocrinology Letters. 2003;24(3-4):233-240.
- Karaa A, Bertini E, Carelli V, et al. Efficacy and safety of elamipretide in individuals with primary mitochondrial myopathy: the MMPOWER-3 randomized clinical trial. Neurology. 2023;101(3):e238-e252.
- ClinicalTrials.gov. A study to evaluate the efficacy and safety of elamipretide in subjects with primary mitochondrial myopathy (MMPOWER-3). Identifier NCT03323749.
- Muzumdar RH, Huffman DM, Atzmon G, et al. Humanin: a novel central regulator of peripheral insulin action. PLoS One. 2009;4(7):e6334.
- Pickart L, Margolina A. Regenerative and protective actions of the GHK-Cu peptide in the light of the new gene data. International Journal of Molecular Sciences. 2018;19(7):1987.
- Liu D, Yu Z, Yin J, et al. The efficacy and safety of thymosin alpha-1 for sepsis (TESTS): multicentre, double blinded, randomised, placebo controlled, phase 3 trial. BMJ. 2025;388:e082583.
- US Food and Drug Administration. FDA warns telehealth companies, online retailers about illegally marketing unapproved versions of semaglutide and tirzepatide.
- US Food and Drug Administration. Research use only products and human use. Warning letters, Center for Drug Evaluation and Research.
Written by Ines Zamora, consumer-health journalist. Reading the studies before believing the pitch. Last reviewed June 2026.
Informational use only. Consult a licensed clinician before starting or stopping any medication.



